close
* 腹痛 + 胰臟酵素上升 = 胰臟炎 ( X )
要考慮 CT 排除其他原因 ( ex : Hallow organ perforation)
Relieved by sitting up
(like pericarditis – can think of pancreatitis as the pericarditis of the belly)
May improve with sitting up with the knees flexed
Trypsin is activated within the pancreatic acinar cells.
leading to pancreatic autodigestion, injury, and inflammation.
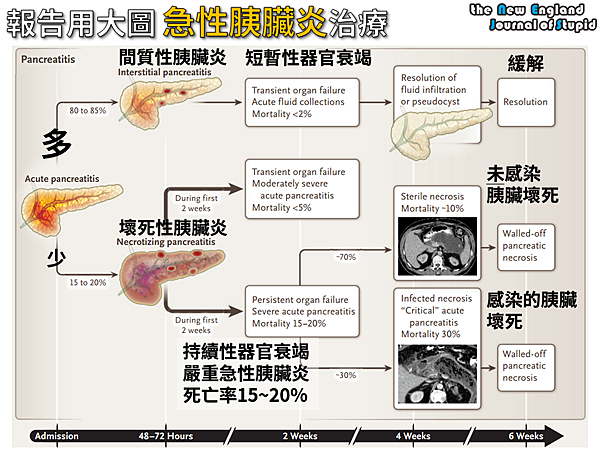
Most cases (~80%) involve only mild inflammation of the pancreas,
a disease state with a mortality rate of < 1%,
which generally resolves with only supportive care
胰臟炎記得找原因 :
Gallstones, CBD stone at ampulla vater
Alcohol
Metabolic : High TG, Hypercalcemia
Infection : Virus (CMV, EBV, adeno, HSV, mumps)
Autoimmune : IgG4
Post ERCP, Trauma
Drug : DPP4 inhibitor
High TG Acute pancreatitis :
症狀較 subacute, amylase & lipase 可能不會高
Medications associated with acute pancreatitis
can be categorized into three groups :
antiretrovirals, chemotherapy, and immunosuppressants.
Diagnosis at least two of three criteria :
(1) Clinical presentation consistent with acute pancreatitis,
(2) Serum lipase or amylase value significantly elevated above the upper limit of normal, or
(3) Imaging findings characteristic of acute pancreatitis
Lab
No gold standard laboratory diagnosis for acute pancreatitis
Difficult to determine applicable levels for older patients or those with multiple comorbidities
Lipase
Sen 90% & Spe 都最高, 和預後無關
Elevated longer than amylase
Elevated in diabetes and some nonpancreatic diseases such as renal disease, appendicitis, and cholecystitis,
it is less associated with nonpancreatic diseases than amylase.
Amylase
Amylase is not a good choice for diagnosis
Peaks within 48 hours, and normalizes in 3 to 5 days
Sen 70% : About 20% of patients with pancreatitis,
most of whom have alcohol- and hypertriglyceridemia-related disease,
will have a normal amylase
Spe 差 (salivary gland, PPU) : renal insufficiency,
salivary gland diseases, acute appendicitis, cholecystitis,
intestinal obstruction or ischemia, and gynecologic diseases,
lowering its specificity for pancreatitis
- ALT > 3倍 : 可能是 Gall stone pancreatitis
Alanine aminotransferase of >150 U/L within the first 48 hours of symptoms
predicts gallstone pancreatitis with a greater than 85% positive predictive value
- False elevation of amylase and lipase in renal failure.
- Lab :
CBC/DC ( Hct ), BUN, Cr
bilirubin, r-GT, Na, K, CRP
Glc, Ca, LDH, GOT/GPT, Gas
Record I/O, body weight, NPO
Anti : flumarin 只用在 necrotizing pancreatitis
Tramal 0.5 amp Q6H + prn, morphine 0.5amp Q4H prn
Hydration : D5S + LR run 180 ml/hr
- CT is often normal within the first 48h
- In patients who meet the clinical presentation and laboratory criteria,
routine early CT, with or without IV or PO contrast, is not recommended
CT findings are delayed compared to clinical presentation
and may underestimate disease severity
complete extent of these local complications is usually not appreciated
until at least 3 days after onset of symptoms.
The magnitude of morphologic change on imaging studies
does not necessarily correlate with disease severity.
治療 :
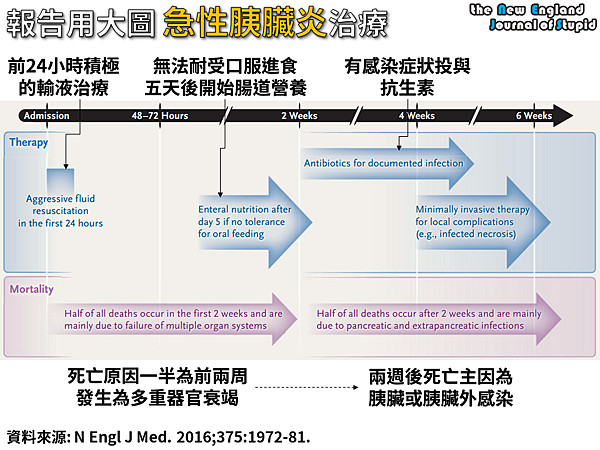
Total of 2.5 - 4 L of fluid over the first 12 to 24 hour
- 輸液輸液輸液 !!!!!
LR at least 250 ml / h
維持 Organ perfusion, UOP > 0.5 / kg / hr
Crystalloid : LR > NS
大量體液流向組織以外, 血管內容積不足
造成 hemoconcetration 與 pre-renal
在診斷急性胰臟炎後12-24hr, 需要大量輸液治療
200-500 mL/hr 是標準建議, 仍需視病人狀況調整
CHF, CKD : deliver fluid more slowly to
prevent complications such as volume overload
- 止痛 : morphine 類會造成 oddi 收縮已被EBM推翻
Pain control is best achieved with IV opioid analgesics.
- NPO :
Initially, place patients on NPO
營養靠週邊 line
預期要很久的可以 TPN
輕微急性胰臟炎,沒有器官衰竭,或非壞死性胰臟炎
不需要到腹痛完全緩解或胰臟酵素恢復正常才開始腸道營養
如果是較嚴重的急性胰臟炎,不能經口營養
五天後可以進行鼻管營養
最佳途徑是 nasojejunal tube
而 nasogastric tube 或 nasoduodenal tube 無顯著差異
- Anti :
* Combined cholangitis
* Necrotizing pancreatitis
* Chronic pancreatitis
* 明顯 abscess formation
Prophylactic use of antibiotics and antifungals is not recommended.
Administer antibiotics if a source of infection is demonstrated,
such as cholangitis, urinary tract infection, pneumonia,
or infected pancreatic necrosis
太多證據顯示"預防性抗生素"對急性胰臟炎病人並無幫助
但現實世界中看到 SIRS
即便沒有很強的感染病徵或病灶,抗生素通常還是下去了
發病兩週後, 感染是另一個關鍵
如果新發生發燒, 白血球飆高, 又開始腹痛, 則要注意這一波的感染
所以另一個用 anti 的狀況是
Necrotizing pancreatitis, 明顯看到 abscess
腹痛一周沒進步變成 chronic
針對腸內菌屬的廣效抗生素
carbapenems 或是第三代 cephalosporins + SABs
- 因為 Bowel perfusion 也差
會 Sentinal bowel loop, Paralytic ileus, N/V
病人開始排氣, 覺得餓, 腸音增加代表往好的方向走
Consider admission for a first bout of acute pancreatitis,
for any case of biliary pancreatitis, and for patients needing frequent IV pain medication,
not tolerating oral intake because of vomiting or increasing pain,
with persistent abnormal vital signs, or with any signs of organ insufficiency
文章標籤
全站熱搜

 留言列表
留言列表

