close
Ischemia bowel = Acute Mesenteric Ischemia (AMI)
腸缺血 = 腸中風
Bowel perfusion 不夠, 造成 Ischemia, Necrosis
考慮 Lactate, D-dimer, VBG, Amylase
CT Triple phase (plain, venous and arterial phase CTs)
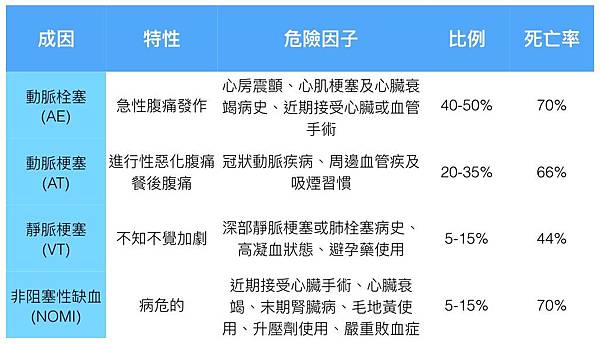
Aterial embolism (50 %)
SMA 最常被塞住
Commonly secondary to cardiac embolic
之前有過 stroke
Af 發生時把 emboli 打出來
也可能是 valve 的 vegetation
Sudden onset abdominal pain, often presents with blood in stool.
Aterial thrombus (10 %)
和其他血管一樣
Atherosclerosis 久了之後塞住 (Atherosclerosis of splanchnic vasculature)
餐後腹痛又稱 Intestinal angina
“Abdominal angina”, commonly presents with post-prandial abdominal pain.
Venous thrombus (10 %)
Often secondary to coagulopathy
高凝血狀態 Active cancer, 腹內感染 ( peritonitis, pancreatitis ), portal HTN, IBD
Non-specific abdominal pain, +/-diarrhea and anorexia.
Non occlusive (25 %)
Non-occlusive Mesenteric Ischemia
沒有塞住, CO 下降, Hypovolemic ...
灌流差引發缺血
Hypoperfusion to mesenteric vasculature due to low cardiac output or splanchnic vasoconstriction.
May have blood in stool.
Common in elderly, septic patients, patients on vasopressors.
Risk Factors for Mesenteric Ischemia
Age > 50
Vascular risk factors
Atrial Fibrillation
Coagulopathy
Low flow state (e.g. septic shock)
Symptoms :
常有 AMI, Stroke, arrhythmia history
Sudden onset abd pain 與觸痛不成比例 (病人覺得很痛, PE 壓起來卻還好 )
Abd distension, N/V, Hematochezia 血便 (muscosa 壞死脫落)
但也有 25 % 不痛 !! 只用 Abd distension 來表現
通常 SMA embolism 會較典型 Sudden onset 超痛
其他原因的可能就 Abd distension 為主, 症狀不太典型
初期腸音還 normal, 之後 fever
後期可能非常脹, 腸音 decrease with diffuse pain
到 peritoneal sign 出現 代表已經 bowel infarction
1. 腹痛期 : 血流供應受阻造成 muscosal 缺血
這樣的腹痛是內臟痛, 模糊的, 可以是絞痛, 也可以是持續痛
但缺血的痛往往又比一般的內臟痛要強烈, 所以會有 "Pain out of proportion"
2. 吐拉期 : 嘔吐及腹瀉是因為腸缺血造成腸道排空 (gut-emptying)
3. 緩解期 : 有些病患接下來可能有 3-6 小時的緩解期
這是因為腸道的神經受缺血的影響而不敏感
4. 壞死期 : 腹痛再度加劇, 因為腸道已全層壞死
這時是體壁痛, 所以會有反彈痛, 肌肉僵硬等腹膜炎現象
腸道內的細菌 translocation 到腹腔及血流造成敗血症及休克
當然這時期有機會看到血便, 甚至看到混著腸道壞死組織的血便
https://emdxhouse.com/
Ischemia bowel 的症狀及徵象不具敏感性及特異性
沒有任何急性腹痛是有機會排除 Ischemia bowel 的
事實上絕大多數的腹痛吐拉, 甚至帶血便的病患只是急性腸胃炎
或更嚴重的感染性腹瀉而已
重要的 Lab 是 FBOT 約有 70 % 初期就 +
Lactate
can be normal early, sensitivity can be as low as 52% depending on stage of disease
do not rely on lactate to rule out mesenteric ischemia
D-dimer
96% sensitivity for mesenteric ischemia In one study – Neg LR = 0.12 -
higher sensitivity than lactate! poor specificity !
Amylase –
can be elevated so don’t be fooled into assuming pancreatitis!
Troponin often elevated & can mislead you to assume AMI
and delay diagnosiss of mesenteric ischemia resulting in higher morbidiy/mortality
Venous Blood Gas – may have metabolic acidosis
Leukocytosis : 75-90% Ischemia bowel 病患其 WBC >15000/uL
乳酸血症 (lactatemia) : 90% 的病患其血中乳酸增加
D-Lactate由細菌產生, 細菌在壞死的腸道中過度生長, 所以對 Ischemia bowel 的敏感性較高
而相反的 L-Lactate 是由人體無氧代謝產生
25% 的病患其腹部 X光是正常的
最常出現的現象是小腸膨脹呈現 Adynamic ileus
當缺血進展, 腸壁水腫或出血時在 X光下腸壁 Thumbprinting
之後進展成 Pneumatosis intestinalis, Portal vein gas
Bowel dilation, Thumb printing,
Ileus, (often misinterpreted as mechanical bowel obstruction),
Pneumatosis in severe cases.
Early CT Findings : non-specific findings -
bowel wall thickening, bowel dilation, mesenteric edema, ascites
Contrast 下 bowel wall poor perfusion
甚至直接看到 大血管內有 thrombus, embolism ~
非常晚期會出現經典的 Pneumatosis intesinalis
腸壁壞死出現 air
之後順著 venous system 回流到 portal vein (Portal vein gas)
最後散在 liver 周邊
CT – Speak with radiology regarding protocol:
Venogram – if suspicion of venous thrombosis
Angiogram – if suspicion of arterial emboli
Triple phase (plain, venous and arterial phase CTs) –
increased sensitivity for mesenteric ischemia; but, increased radiation exposure
要去 D/D 排除 ileus, Hallow organ peforation !
Fluid resuscitation :
can have massive 3rd space losses, +/- bleeding.
Aggressive IV fluid resuscitation often required.
Antibiotics : consider broad spectrum antibiotics if patient presents with a septic picture
Anticoagulation (controversial) :
if embolic source, no urgent OR, and no bleeding, consider heparin
Early surgical consult
Vasopressors :
try to avoid vasopressors in mesentric ischemia as they may worsen ischemia,
but if required,
choose pressors with least effect on splanchnic circulation (i.e. dobutamine/ milrinone).
Avoid epinephrine, phenylephrine because of vasoconstrictive effects.
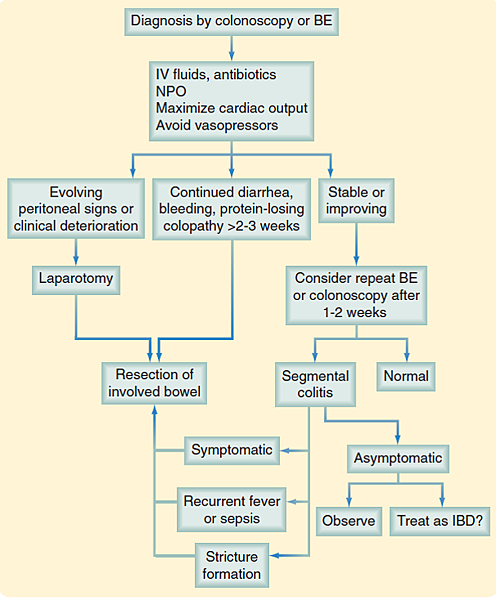
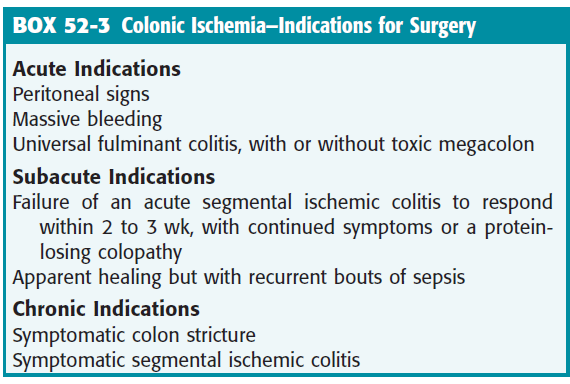
Ischemic colitis
Cramping LLQ pain + Diarrhea + 明顯 Bloody stool +/- Fever
到 infarction 時會出現 peritoneal sign
Hyperactive phase occurs first,
the primary symptoms are severe abdominal pain and bloody stools.
Many patients get better and do not progress beyond this phase.
Paralytic phase can follow if ischemia continues,
the abdominal pain becomes more widespread
the belly becomes more tender to the touch,
and bowel motility decreases, resulting in abdominal bloating,
no further bloody stools, and absent bowel sounds on exam.
Finally, a shock phase can develop
as fluids start to leak through the damaged colon lining.
Most common early signs of ischemic colitis include
abdominal pain (often left-sided)
with mild to moderate amounts of rectal bleeding
第一次解血便前, 會先有劇烈腹痛
之後是無痛性的解血便
通常會陸陸續續的解好幾次
有一定血量, 但很少解大量血便或休克
看診時病人肚子不會痛
生命徵像穩定
理學檢查正常沒有腹部壓痛
血液 CBC, 生化, PT/aPPT 也都正常
常誤以為是 hemorrhoid出血
好發在降結腸
典型的超音波影像會出現一段的下降結腸腫脹或腸壁變厚
Segmental swelling or wall thickening of descending colon
結腸腫脤變厚的程度, 決定於發病的時間和缺血的嚴重程度
一般來說, 發病時間越長或缺血越嚴重的個案
超音波影像較容易辨視
但輕症的病人, 僅會出現不腫不厚的結腸
Elderly
Mesenteric vessels artherosclerosis
Embolic disease, Vasculitis, DIC
Hypovolemic or endotoxic shock
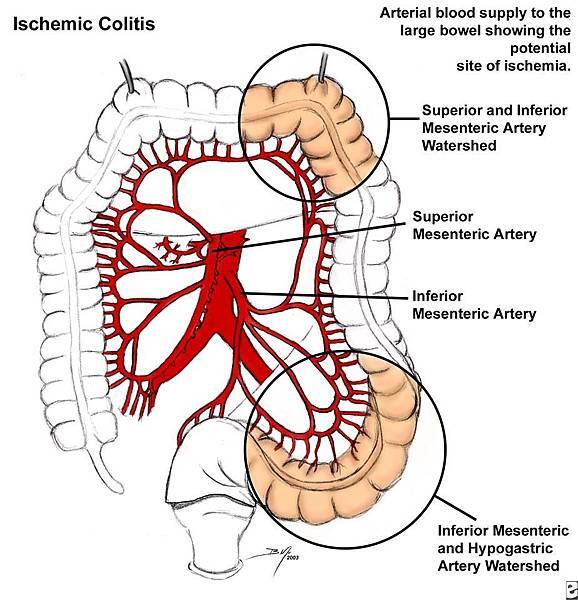
Watershed region :
- Splenic flexure
- Rectosigmoid junction

Mucosa : May be transient and recovery may be complete.
Muscularis : Scarring and a chronic stricture
Full thickness : May result in gangrene, with perforation and fecal peritonitis.
Plain film (Often nonspecific)
- Ileus
- Isolated segment of distended colon
- Thumbprinting (intestinal wall edema or submucosal hemorrhage)
- Free intraperitoneal air
Colitis :
Infectious : Clostridium, Shigella, EHEC, parasite
Ischemic
Autoimmune - IBD
Idiopathic
Shigella 志賀 :
人傳人, S. sonnei 常見, S. dysenteriae 造成嚴重疾病
1-10菌就可致病, shigella 會侵入黏膜下層造成 嚴重血便
少數會導致 HUS 溶血性尿毒
EHEC :
腸出血性大腸桿菌 :
人傳人 其中 O157 可製造 shiga-like toxin 造成 HUS
攻擊大腸造成出血性大腸炎, 攻擊腎臟造成腎衰竭 uremia
C. difficile 艱難梭菌 :
厭氧 GPB, 因為 clindamycin 之使用造成
pseudomembranous colitis
口服 metronidazole or vanco
全站熱搜

 留言列表
留言列表

