close
大流程 :
Line * 2
VBG/ABG : Acidosis or not
CBC/DC, Na, K, Ca, Cl, Ketone, Creatinine
EKG r/o AMI, HyperK
U/A, CXR r/o infection
Line 1 :
Bolus RI 0.1 U/kg IVP
then run 0.1U/kg/hr
(50U in NS 500 ml : 幾公斤就 run 幾 ml)
Line 2 :
NS challenge 10-15 ml/kg/hr, then run 2 ml/kg/hr
80-150 ml/hr based on fluid status
(成人第一小時平均需要 1-2 L ; 兒童第一小時 10-20 ml/kg
F/u F/S, ABG : Q2H*2 -> Q4H *2 -> 4 段 or Q8H
F/u Na, K, Cl : Q4H -> Q8H
Underlynig 6I should be solved !!
- K < 3.3 : Hold insulin + 先補鉀
- K > 5.3 : 才不用補鉀
- pH < 6.9 才補 Bicarbonate
- 血鈉校正後, 決定給 N/S or H/S
Diabetic Ketoacidosis in End Stage Renal Failure Patient On Maintenance Dialysis –
Key Challenges in Management
However, in ESRF, especially aneuric one who depend on regular dialysis,
treatment could pose a challenge as they can easily go into fluid overload with fluid replacement,
insulin tend to remain longer in body due to reduced renal excretion,
and potassium replacement may not be required as per non-dialysis patients.
Unlike normal population,
maintenance potassium is not required as ESRF patients tend to have hyperkalaemia.

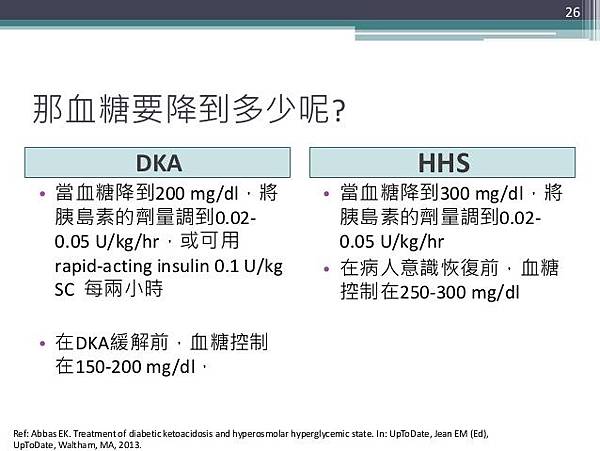
→ 目標的降血糖速率:50-75 mg/dL/hr
→ 如果 >100mg/dL/hr, 可能會增加 osmotic encephalopathy
測到的 Na 要 Corrected (Glucose 每 ↑ 100 mg/dL ↓ 1.6 or 2.4 Na)
雖然 dehydration 會讓血鈉高
但身體多出額外的 Osmole (Glucose) 會把水從細胞內拉出來
會使測得 Na 比真實狀況更低
** Corrected Na = Measured Na + 2.4 or 1.6 * (Measured Glucose -100)/100 **
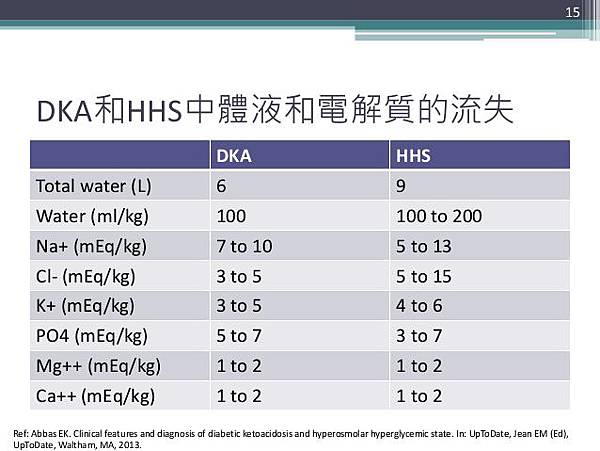
嚴重缺鉀 (300-600 mEq)
滲透性利尿就會流失鉀離子
Dehydration 使 Aldo 會留鈉排鉀
身體基本上是缺鉀的
但 Acidosis, insulin deficiency 會使鉀 shift 出胞外
Dehydration 也會使測到的鉀濃度變高
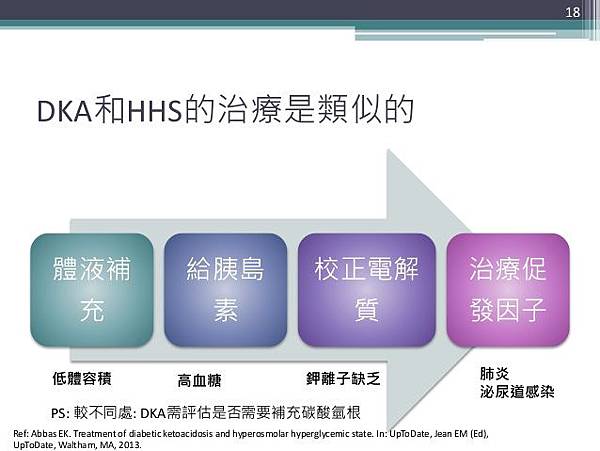
* DKA key point : Insulin
* 治療目標 : No acidosis, No ketone bodys
血糖不是重點, 只要不要低血糖就好
就怕 Insulin 給的不夠多不夠久
即使 sugar 正常了 還是要給 IV insulin + D5D10W (避免低血糖)
太早停掉 insulin 會反覆 DKA
文章標籤
全站熱搜

 留言列表
留言列表

